Menu
HOME
ABOUT US
SERVICES
HOSPITAL FEASIBILITY STUDY
HEALTHCARE FACILITY PLANNING AND DESIGN
MEDICAL EQUIPMENT PLANNING CONSULTANTS
GLOBAL HEALTHCARE CONSULTING FIRM
CORPORATE SOCIAL RESPONSIBILITY (CSR)
DIGITAL HEALTH SOLUTIONS
END TO END - TURNKEY SOLUTIONS
DESIGN OF BOUTIQUE HEALTHCARE CENTRES
INNOVATIONS
STEPS OF HOSPITAL PLANNING
ACCREDITATION COMPLIANT (NABH & JCI)
HEALTHCARE DUE DILIGENCE STUDY
HOSPITAL PROJECT REPORT
IMPACT OF COLORS IN HOSPITAL DESIGN
GREEN HOSPITALS
LEAN & SMART HOSPITALS
DESIGNING HOSPITALS TO BE PATIENT FRIENDLY
HOSPITAL PROJECTS WORKSHOP
NEWS
CLIENTS
CAREERS
CONTACT
Toggle navigation
Menu
HOME
ABOUT US
SERVICES
HOSPITAL FEASIBILITY STUDY
HEALTHCARE FACILITY PLANNING AND DESIGN
GLOBAL HEALTHCARE CONSULTING FIRM
MEDICAL EQUIPMENT PLANNING CONSULTANTS
CORPORATE SOCIAL RESPONSIBILITY (CSR)
DIGITAL HEALTH SOLUTIONS
END TO END - TURNKEY SOLUTIONS
HOSPITAL PLANNING ONLINE SEMINAR
INNOVATIONS
STEPS OF HOSPITAL PLANNING
ACCREDITATION COMPLIANT (NABH & JCI)
HEALTHCARE DUE DILIGENCE STUDY
HOSPITAL PROJECT REPORT
IMPACT OF COLORS IN HOSPITAL DESIGN
GREEN HOSPITALS
LEAN & SMART HOSPITALS
DESIGNING HOSPITALS TO BE PATIENT FRIENDLY
HOSPITAL PROJECTS WORKSHOP
CLIENTS
CAREERS
CONTACT US
Home
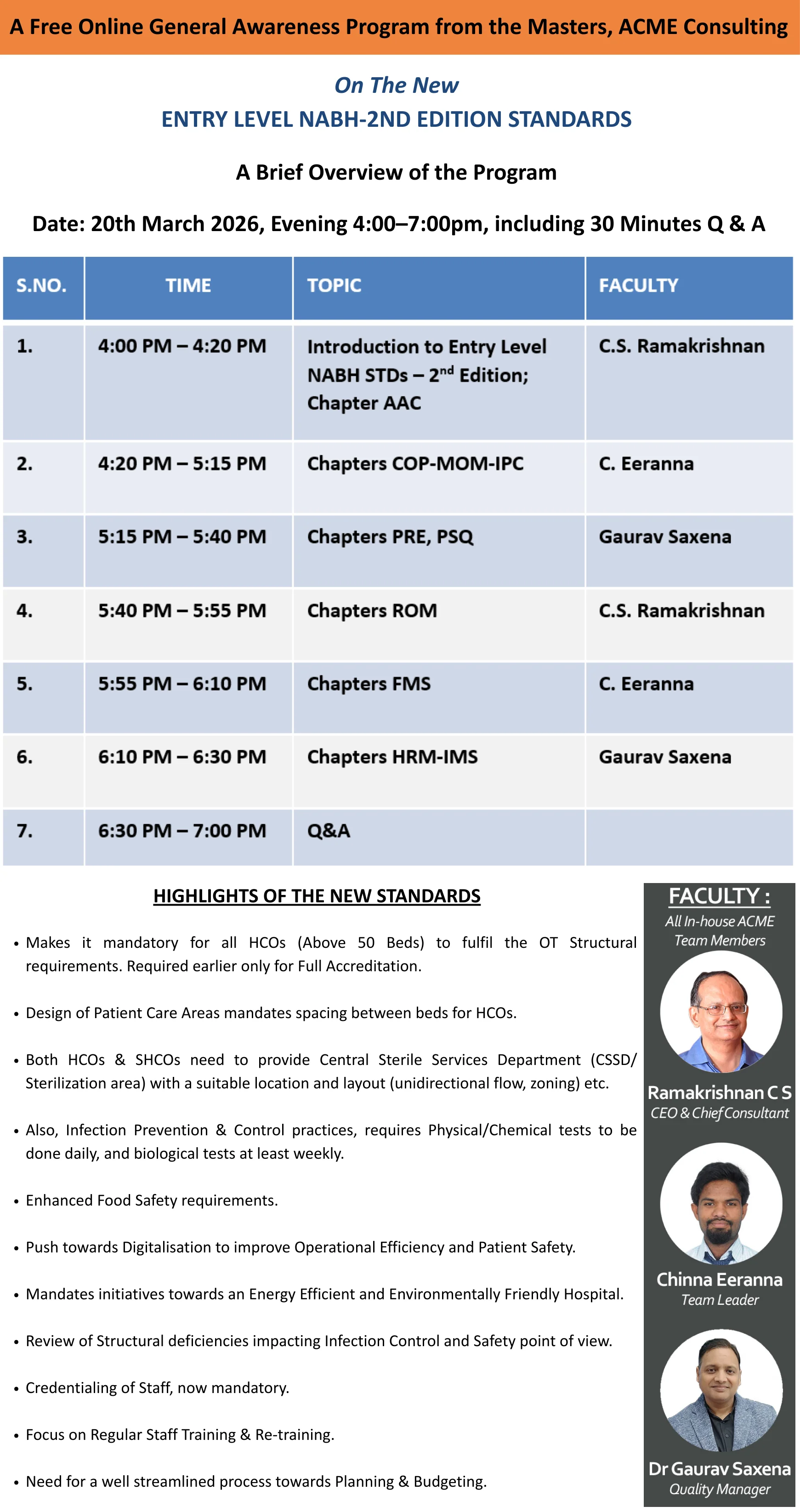
>> NABH Training Program
Please fill up the form shown below to help us confirm your registration.
Your Name*
:
Hospital / Institution Name*
:
Phone Number*
:
Email id*
:
Address*
:
SUBMIT